Introduction:
Concussion, which is a mild form of traumatic brain injury (mTBI) has an incidence of 1.6 to 3.8 million sports related concussions per year. Outside of sport the leading causes of TBI are falls, motor vehicle crashes, struck by or against events, and assaults, respectively. The International Conference on Concussion in Sport defines concussion as “a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces. Several common features that incorporate clinical, pathological, and biomechanical injury constructs that may be used in defining the nature of a concussive head injury include the following:
1) Concussion may be caused by a direct blow to the head, face, neck or somewhere else on the body with an impulsive force transmitted to the head
2) Concussion typically results in the rapid onset of short lived impairment of neurological function that resolves spontaneously.
3) Concussion may result in neuropathilogical, but the acute clinical symptoms largely reflect a functional disturbance rather than structural injury.
4) Concussion results in a grade set of clinical syndromes that may or may not involve loss of consciousness. Resolution of the clinical and cognitive symptoms typically follows a sequential course.
5) Concussion is typically associated with grossly normal neuro-imaging studies.
The accepted time frame for recovery is not scientifically established, but is influenced by factors such as age, sex, and history of prior concussions. Although the vast majority of patients who sustain a concussion will reach full neurological recovery within 1-2 weeks, 15-20% will demonstrate persistent signs and symptoms lasting greater than 3 weeks. The post-concussion syndrome refers to a large number of symptoms and signs that may occur alone or in a combination following mild head injury. The most common complaints are headaches, dizziness, fatigue, irritability, anxiety, insomnia, loss of consciousness and memory, and noise sensitivity.
Clinical studies in patients with whiplash-type injuries and concussion and experimental studies with animals humans have established the important role of the cervical spine in mediating balance, head orientation and eye movement. The high density and complexity of muscle and joint mechanoreceptors throughout the cervical spine are a rich source of proprioceptive information that is conveyed to multiple levels of the CNS, including the cerebellum, brainstem, and spinal cord.
Some authors have observed significant improvements in neck pain, range of motion and disability in patients with whiplash when comprehensive programming targeting cervical joint position re-training, and balance were applied.
Methods:
The initial procedure in the study was a thorough history taking to confirm that each patient had a concussion and was suffering from post-concussion symptoms for at least 6 weeks. An examination was then done to determine if there was evidence of an upper cervical subluxation. The examination procedure was as follows:
1) Postural assessment looking for evidence of head tilt, shoulder un-levelling, pelvic un-levelling.
2) Supine leg check looking for evidence of a short leg.
3) Bilateral weight scales looking for evidence of a significant shift of weight to one side.
4) Spinal palpation assessing spinal range of motion, spinal fixations, changes in muscle tone, changes in tissue tone.
5) Infra-red para spinal thermography, assessing for significant thermal asymmetries.
6) Upper cervical orthogonal based x-rays to measure for significant upper cervical misalignment
When it was determined that an upper cervical subluxation was present the patients filled out the post-concussion intake questionnaires. The questionnaires were as follows: The Rivermead Post Concussion Questionnaire (1) , The neck disability index, the headache disability index, the dizziness handicap inventory and the Rand SF-36. They filled out the same forms at week 6 and week 12 to compare the findings.
Following this, chiropractic care began and a chiropractic adjustment was performed to restore proper alignment and function to the upper cervical spine. Following the first adjustment post x-rays were done to confirm that a correction had been made.
The patients were monitored over the next 12 weeks to determine if they were holding their correction or whether another adjustment had to be performed. This was done using the following 5 procedures at each visit:
1) Postural assessment looking for evidence of head tilt, shoulder un-levelling, pelvic un-levelling.
2) Supine leg check looking for evidence of a short leg.
3) Bilateral weight scales looking for evidence of a significant shift of weight to one side.
4) Spinal palpation assessing spinal range of motion, spinal fixations, changes in muscle tone, changes in tissue tone.
5) Infra-red para spinal thermography, assessing for significant thermal asymmetries.
When it was determined that a subluxation was present the patient was adjusted using the Nucca procedures. The patients were placed side posture on the Nucca adjusting table and a specific force was directed into the transverse process of the Atlas at the predetermined specific vector. Once the adjustment was accomplished they rested for a minimum of 10 minutes on a bed to allow the body to process the adjustment. They were then re-checked using the 5 parameters above to see that a correction had been made.
The frequency of visits ranged from weekly to three visits per week depending on how well the patient was holding their adjustment.
Results:
From initial assessments 8 patients were eligible for inclusion. After the initial stage of care 2 patients did not meet the inclusion criteria. One patient was unable to complete care due to personal issues and the other patient suffered 2 concussions during the study.
Six patients (4 female,2 male) were included in the study, age range from 39 to 82, average age of 56. The duration of post-concussion symptoms ranged from 6 weeks to 14 months duration, with the average being of 7 months duration. There were no changes in medication and no other therapies were used or started through the duration of the study.
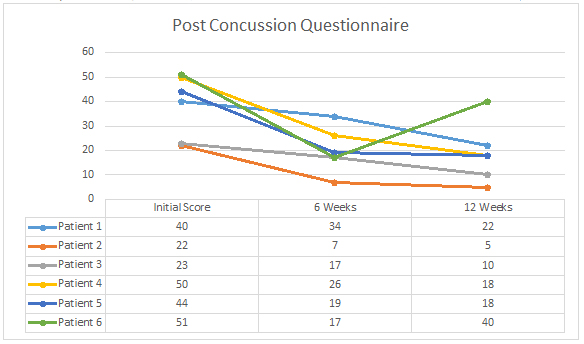
The Rivermead Post-Concussion Questionnaire showed an improvement in scores in all 6 patients. (see Table 1) In the initial 6 weeks of care the average improvement was 18 points with the range being between 6 and 34 points. As a percentage, there was an average of 47% improvement in the first 6 weeks, with a range of 15% to 68%. Five of the six patients showed continued improvement between week 6 and week 12, while patient 6 showed a regression back towards original values. The average improvement for the 5 patients between week 6 and 12 was 6 points, while the 6th patient reverted by 23 points. From the beginning of the study to the completion the average improvement for all 6 patients was 19.5 points. As a percentage that works out to be a 54% improvement, with a range of 21% to 77%.
|
Table 1: (Click on graph to enlarge) |
 |
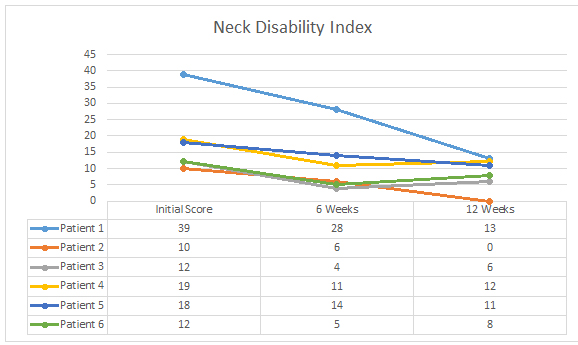
The neck disability index showed an improvement in scores in all 6 patients.(see Table 2) In the 12 weeks of care the average improvement was 54%, with a range of improvement from 33% to 100%. There was on average a 10 point change in the 6 patients which is considered to be clinically significant. ↑ Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM, Childs JD. Responsiveness of the Neck Disability Index in patients with mechanical neck disorders. Spine, 2009 Jul 24, online article ahead of print.
|
Table 2: (Click on graph to enlarge) |
 |
The headache disability index showed an improvement in 5 out of 6 patients, with the 6th patient exhibiting no headaches throughout the study. (see Table 3) There was on average a 19 point improvement in the 5 patients exhibiting headaches, with the range being 4 to 38 points. As a percentage, there
was a 51% improvement in headaches on average, with a range of improvement being 23% to 67%. Although this is a statistically significant decrease in scoring over the 12 weeks it should be treated with caution since an improvement of 29 points is considered to be clinically significant.(2) The relatively large change necessary for clinical significance limits the robustness of the test as subjects initially reporting moderate disability scores must virtually eliminate associated disability and those with scores below this value are limited by a basement effect.(3)
|
Table 3: (Click on graph to enlarge) |
 |
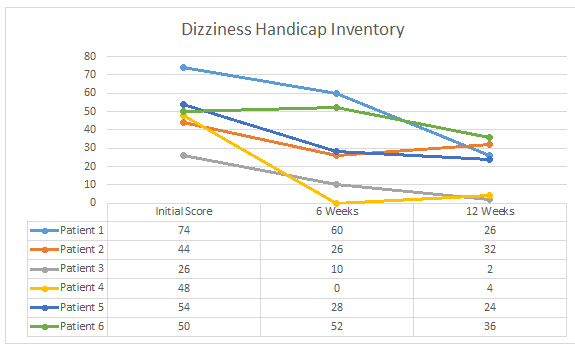
The dizziness handicap inventory showed an improvement in all 6 patients over the 12 weeks. (see Table 4) The average improvement was 29 points, with a range of 12 to 48 points. As a percentage this is a 60% improvement on average, with a range of 27% to 92%. This is considered to be a clinically significant improvement in vestibular rehabilitation, which requires an improvement of 18 points to be significant. (4)
|
Table 4: (Click on graph to enlarge) |
 |
Patient Histories:
Patient 1:
A 59 year old female. She suffered a concussion 6 weeks earlier from running into the edge of a door. Her symptoms included constant headaches, photophobia, increased sound sensitivity, anxiety, nausea and tinnitus. Prior history included a severe whiplash 30 years earlier with a history of headaches.
After 12 weeks of care she could go without sunglasses inside, could tolerate sound, was much more relaxed, better moods, could think clearer, less headaches, improved blood pressure, less neck pain and better balance.
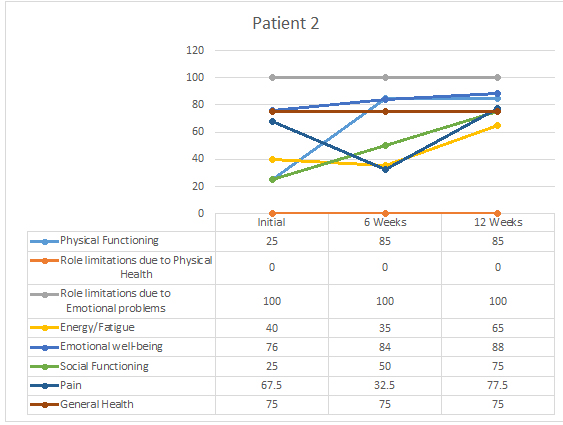
Patient 2:
A 53 year old male. He suffered a concussion 12 weeks earlier from falling backwards and banging his head on the ice while playing hockey. His symptoms included photophobia, mental fogginess, low energy, poor sleep, poor balance, pressure in head, neck/shoulder pain, difficulty concentrating.
After 12 weeks of care he was able to work full time again, had less neck/shoulder pain, more energy and improved sleep. He had decreased head pressure but it would come and go and still had poor balance.
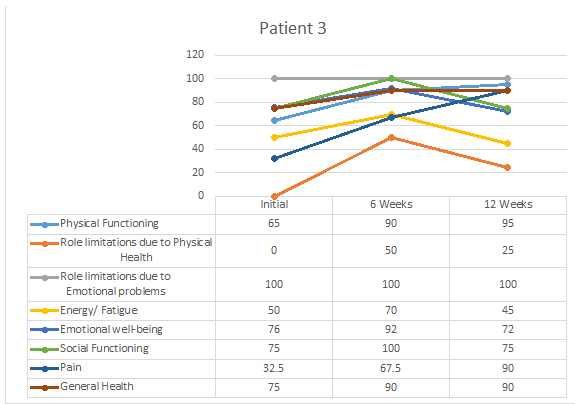
Patient 3:
A 43 year old female. She suffered a concussion from 3 separate accidents over a 5 week period, 10 months prior to coming in. She was initially rear-ended in a car accident, then fell down the stairs 1 week later and then fell on the back of her head a month later skiing. Her symptoms included constant neck pain, frequent headaches, difficulty concentrating, frequent dizziness, sinus congestion, low energy, eye pain and difficulty focusing, and difficulty exerting while exercising.
After 12 weeks of care she reported significantly less neck pain and headaches, less dizziness, clearer sinuses, clearer vision and less eye pain, better concentration and energy, able to write reports at work again and exert with exercising.
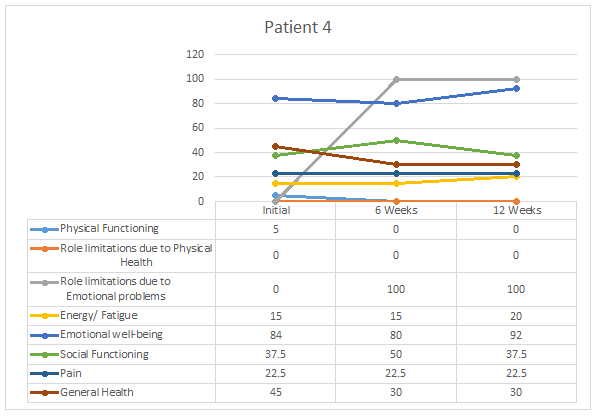
Patient 4:
An 82 year old female. She suffered a concussion 3 months earlier when she fell and banged her head behind the left ear on a door jamb. Her symptoms included shooting pains in her head, neck pain, dizziness, low energy, frequent nausea, headaches and poor sleep.
After 12 weeks of care she reported less neck pain, no dizziness, better sleep and feeling more restful.
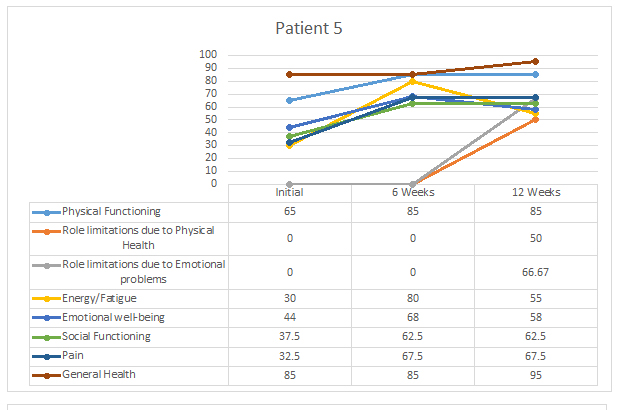
Patient 5:
A 39 year old male. He suffered a concussion 11 months earlier after being hit in the side of the head during a Muy Thai match (martial arts). His symptoms included constant headaches and neck pain, mental fogginess, sinus pain and head pressure, ear sensitivity, heart rhythm irregularity, inability to exert with exercise, poor sleep, tinnitus.
After 12 weeks of care he reported a decrease in headaches, dizziness and neck pain.
Patient 6:
A 59 year old female. She suffered a concussion 14 months earlier after a hard fall, in which she was unconscious for 20 minutes. Her symptoms included poor concentration, brain fogginess, fatigue, marked dizziness, blurry vision, sinus congestion, poor sleep and decreased coordination.
After 12 weeks of Chiropractic care she reported having more energy, better moods, better sleep, a much clearer mind, clearer sinuses, clearer vision, far less dizziness, and better coordination.
Discussion:
In this limited cohort of 6 post-concussion patients there were statistically and clinically significant improvements in many of the indexes studied after the NUCCA intervention.
Part of our original hypothesis assumes that trauma significant enough to cause post-concussion syndrome can also significantly influence cervical spine function. This is seen in our findings. The neck disability index showed clinically significant changes following the 12 weeks of NUCCA Chiropractic care. The correlation between restoring cervical spine function and improvements in post-concussion symptoms can be seen in other studies as well (6,7) and points to the importance of therapy in this area.
Headaches are a common symptom of post-concussion syndrome(9) and in this study 4 out of the 6 patients had headaches on a regular basis. In one study on 452 patients with traumatic brain injuries over 41% of patients continued to have headaches at the 3,6, and 9 month intervals following the trauma.(9) In another study on 212 patients with mild traumatic brain injury there was a headache rate of over 58% at the 3, 6 and 9 month interval following trauma.(10) In this study there were statistically significant changes in all the patients that had headaches on a regular basis. The correlation between headaches and the upper cervical spine has been found in many studies(11,12,13). This correlation suggests that a significant proportion of post-concussion headaches could relate to upper cervical spine function.
It has been reported that dizziness is a common aspect of post- concussion with studies showing that 43-81% of sports related concussions include dizziness.(15,16) All 6 patients in this study were experiencing dizziness to some degree and the improvements were clinically significant following Nucca Chiropractic care. This highlights the importance of addressing the cervical spine function with post-
concussion patients. It has been found that restoring cervical spine function with manual therapy and/or Chiropractic adjustments can significantly help with dizziness. (17,18)
Post Concussion Findings:
| Rivermead Post - Concussion Questionnaire: | Initial score | 6 weeks | 12 weeks |
| Patient 1 | 40 | 34 | 22 |
| Patient 2 | 22 | 7 | 5 |
| Patient 3 | 23 | 17 | 10 |
| Patient 4 | 50 | 26 | 18 |
| Patient 5 | 44 | 19 | 18 |
| Patient 6 | 51 | 17 | 40 |
| Neck Disability Index | Initial score | 6 weeks | 12 weeks |
| Patient 1 | 39 | 28 | 13 |
| Patient 2 | 10 | 6 | 0 |
| Patient 3 | 12 | 4 | 6 |
| Patient 4 | 19 | 11 | 12 |
| Patient 5 | 18 | - | 11 |
| Patient 6 | 12 | 5 | 8 |
| Headache Disability Index | Initial score | 6 weeks | 12 weeks |
| Patient 1 | 38 | 36 | 14 |
| Patient 2 | 44 | 38 | 34 |
| Patient 3 | 36 | 20 | 18 |
| Patient 4 | 6 | 0 | 2 |
| Patient 5 | 72 | 40 | 34 |
| Patient 6 | 0 | 0 | 0 |
| Dizziness Handicap Inventory | Initial score | 6 weeks | 12 weeks |
| Patient 1 | 74 | 60 | 26 |
| Patient 2 | 44 | 26 | 32 |
| Patient 3 | 26 | 10 | 2 |
| Patient 4 | 48 | 0 | 4 |
| Patient 5 | 54 | 28 | 24 |
| Patient 6 | 50 | 52 | 36 |
Rand SF-36 Values:
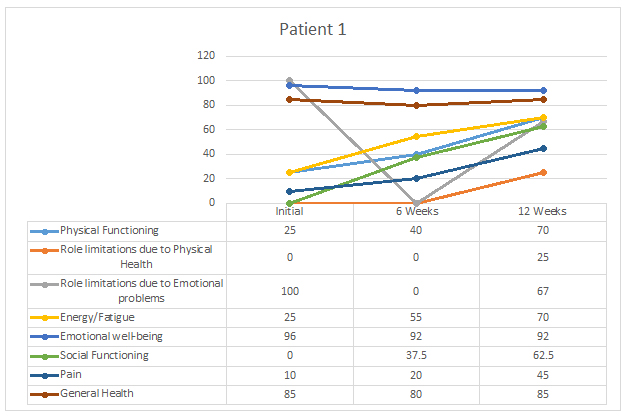
| Patient 1 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 25 | 40 | 70 |
| Role Limitations due to Physical Health | 0 | 0 | 25 |
| Role Limitations due to Emotional Health | 100 | 0 | 67 |
| Energy/Fatigue | 25 | 55 | 70 |
| Emotional Well-Being | 96 | 92 | 92 |
| Social functioning | 0 | 37.5 | 62.5 |
| Pain | 10 | 20 | 45 |
| General Health | 85 | 80 | 85 |
| Patient 2 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 25 | 85 | 85 |
| Role Limitations due to Physical Health | 0 | 0 | 0 |
| Role Limitations due to Emotional Health | 100 | 100 | 100 |
| Energy/Fatigue | 40 | 35 | 65 |
| Emotional Well-Being | 76 | 84 | 88 |
| Social functioning | 25 | 50 | 75 |
| Pain | 67.5 | 32.5 | 77.5 |
| General Health | 75 | 75 | 75 |
| Patient 3 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 65 | 90 | 95 |
| Role Limitations due to Physical Health | 0 | 50 | 25 |
| Role Limitations due to Emotional Health | 100 | 100 | 100 |
| Energy/Fatigue | 50 | 70 | 45 |
| Emotional Well-Being | 76 | 92 | 72 |
| Social functioning | 75 | 100 | 75 |
| Pain | 32.5 | 67.5 | 90 |
| General Health | 75 | 90 | 90 |
| Patient 4 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 5 | 0 | 0 |
| Role Limitations due to Physical Health | 0 | 0 | 0 |
| Role Limitations due to Emotional Health | 0 | 100 | 100 |
| Energy/Fatigue | 15 | 15 | 20 |
| Emotional Well-Being | 84 | 80 | 92 |
| Social functioning | 37.5 | 50 | 37.5 |
| Pain | 22.5 | 22.5 | 22.5 |
| General Health | 45 | 30 | 30 |
| Patient 5 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 65 | 85 | 85 |
| Role Limitations due to Physical Health | 0 | 0 | 50 |
| Role Limitations due to Emotional Health | 0 | 0 | 66.67 |
| Energy/Fatigue | 30 | 80 | 55 |
| Emotional Well-Being | 44 | 68 | 58 |
| Social functioning | 37.5 | 62.5 | 62.5 |
| Pain | 32.5 | 67.5 | 67.5 |
| General Health | 85 | 85 | 95 |
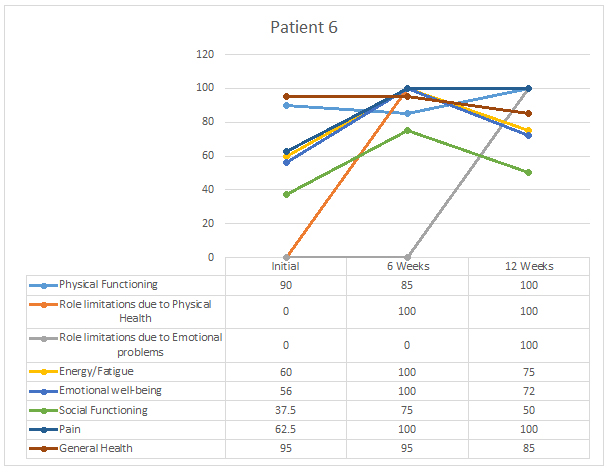
| Patient 6 | Initial | Week 6 | Week 12 |
| Physical Functioning: | 90 | 85 | 100 |
| Role Limitations due to Physical Health | 0 | 0 | 100 |
| Role Limitations due to Emotional Health | 0 | 0 | 100 |
| Energy/Fatigue | 60 | 100 | 75 |
| Emotional Well-Being | 56 | 100 | 72 |
| Social functioning | 37.5 | 75 | 50 |
| Pain | 62.5 | 100 | 100 |
| General Health | 95 | 95 | 85 |
|
Patient 1: (Click on graph to enlarge) |
 |
|
Patient 2: (Click on graph to enlarge) |
 |
|
Patient 3: (Click on graph to enlarge) |
 |
|
Patient 4: (Click on graph to enlarge) |
 |
|
Patient 5: (Click on graph to enlarge) |
 |
|
Patient 6: (Click on graph to enlarge) |
 |
X- Ray Results:
| Atlas Laterality | Rotation | Head Tilt | Lower Angle | Angular Rotation | ||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Patient 1 | L2.8 | L1.3 | A3.9 | A3.6 | R3.2 | R1.9 | R0.2 | L0.8 | R5.9 | R4.0 |
| Patient 2 | L3.3 | L3.5 | A0.3 | ---- | L1.7 | L1.5 | R0.5 | R1.7 | R1.2 | R0.7 |
| Patient 3 | R1.4 | R1.1 | P3.2 | ---- | R3.3 | R1.4 | L2.7 | L0.5 | R4.6 | R0.8 |
| Patient 4 | L0.7 | R0.7 | P4.6 | P3.0 | R0.3 | R1.8 | R5.8 | R3.0 | L4.8 | L1.9 |
| Patient 5 | R2.8 | R1.9 | P0.8 | ---- | R1.2 | R0.6 | L2.5 | L2.2 | R0.9 | R0.9 |
| Patient 6 | R0.6 | R0.8 | A2 | A0.5 | L2.6 | L2.5 | L3.1 | L3.7 | L0.2 | R0.4 |